

Clinical Scenario
First consultation - With a first surgeon
At the age of 15, the patient received two implants subcutaneously:
- a right subcutaneous breast implant, pre-filled with silicone gel, through the periareolar way;
- a standard implant in silicone gel, through the axillary way, in the subclavicular position.
Two months later the subclavicular implant had to be removed due to complications. It had moved from its original position and had ruptured during the attempt of repositioning it. It had been removed through the same incision. The breast implant remained in place.
Second consultation - With Dr Schirmer
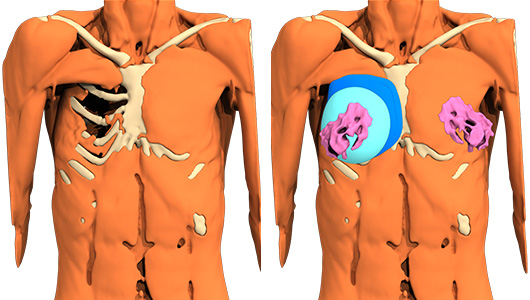
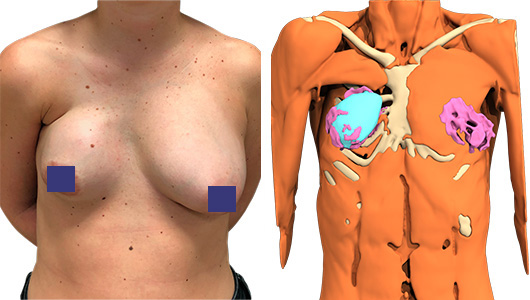
Due to the insufficient result of her first procedure, the patient saw Dr Schirmer at the age of 33. Clinical examination shows a persistence of the chest deformity due to the absence of pectoralis major muscle and a retractile shell deforming the breast implant. The scar is unsightly.
The surgery
The surgery with custom-made implants
The patient chose a new surgery including two operating stages:
- placement of a custom-made elastomer thoracic implant made with computer-aided design (CAD);
- replacement of the breast implant.
First re-intervention
Three months after the consultation, the first re-intervention is performed under general anesthesia:
- passage through the axillary way with a S-shape incision without using the previous way;
- dissection with little bleeding, allowing to create a compartment in contact with the chest wall;
- positioning of the custom-made implant leaving the old breast prosthesis on the front and the thick fibrous capsule surrounding it;
- simple closure of the skin in two planes, no drain necessary.
Surgical follow-up
Simple and painless follow-up (paracetamol), no puncture necessary in the absence of post-operative sero-hematic collection.
The patient is discharged the following day.
Second re-intervention 6 months later
Change of the breast implant through the axillary way: the capsular fibrous plane is respected behind to maintain a partition between the two implants and prevent slipping one over the other.
A new and larger compartment is created on the front for the new soft breast implant, filled with silicone gel. Remodeling of the tuberous and ptosis left breast with periareolar dermo-mastopexy.
Symmetrical repositioning of the areola of the right breast.
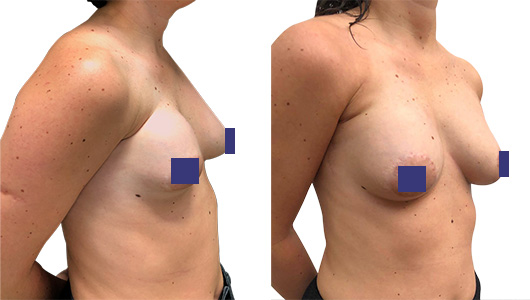
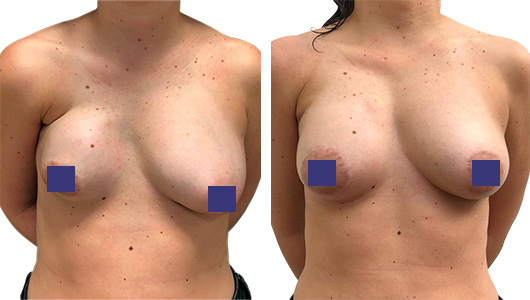
Result
The immediate result is very satisfactory for the patient. Thoracic and breast symmetry is much improved.
Author
Dr Claudia Schirmer is a plastic, aesthetic and reconstructive surgeon as well as a pediatrician. She works at the Italian Hospital of Buenos Aires in Argentina. She is also a member of the Argentinian Society of Plastic Surgery.

